The event began with a discussion of what people hoped to achieve. Participants noted:
The group discussed the social determinants of health (SDOH) as they understood the term and what indicators could be used to measure them. They recognized that indicators and data were critical to any work on community development or health because you are what you measure, and they expressed the desire to share data more cohesively between organizations. The table presents a summary of the key social determinants discussed and the indicators that could be used to measure them. Participants noted that indicators do not always capture the full picture. Two examples given were transportation and childcare. Access to transit does not tell you if health care or jobs are close to transit, it merely tells you if the person has access to transit. In childcare, you may measure outcomes for the child when measuring teacher certifications or tenure, but often miss outcomes for a parent such as a parent’s ability to maintain a job.
Social Determinants of Health and Their Indicators
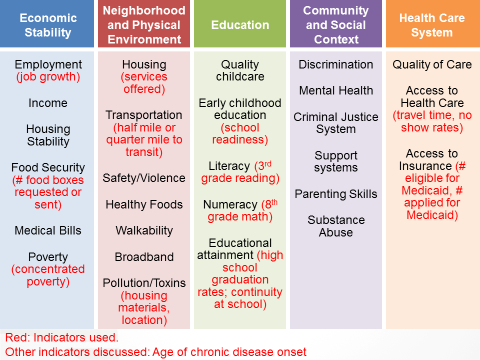
The table does not capture every SDOH discussed at the meeting, but instead provides a selection of determinants and indicators discussed.
Participants then moved into smaller groups to discuss strategies for breaking silos and facilitating cooperation across sectors to tackle the upstream factors affecting health. They then reported their top recommendations on how to best break barriers to address the social determinants of health. These recommendations included:
Participants then discussed possible opportunities for improving their work to address social determinants of health. This included impact mapping to demonstrate the benefits that investments in one silo may have for outcomes in another as well as a “money map” to outline the costs in the systems and the flow of funds through it. The goal would be to demonstrate to policymakers, and possibly to funders, that they do not have an either/or choice between, for example, health and education when it is possible to quantify how an educational investment improves health outcomes. Ideally, this mapping will also identify windows of opportunity available, given participants’ time and resources.
The group discussed the importance of identifying shared goals at the start, and using those common goals to identify practices that could be imported from other parts of the country. However, they acknowledged that any efforts needed to be cognizant of larger macro forces that will be shaping the local contexts, including inequality and rural depopulation, and developing resiliency to these macro forces.
Questions were raised on the geographic scale to consider tackling, with debates on whether it was better to take on statewide projects or issues versus focusing on smaller, more circumscribed geographies. Transportation was an example of an issue that affects people statewide, even though the solution sets for rural and urban areas may not look the same. The group also noted that what are considered best practices must be adaptable to the context of a given place. Finally, participants continued to debate what frame was most useful to garner broad-based support for these issues—whether it was health, opportunity, fiscal efficiency, or others—and whether health should be a hub or a spoke in any efforts here.
Areas that participants wanted to explore further and learn more about as a possible follow-up step included:
Participants also recommended the future inclusion of several additional stakeholder groups, including:
Finally, participants offered some additional next-step recommendations via email, including:
Appendix A: List of SDOH-Related Efforts
At the meeting, participants discussed the following range of efforts they were engaged in related to SDOH:
Madelyn Adams
Director of Community Benefit
Kaiser Permanente
Leigh Alderman
Senior Adviser
Georgia Health Policy Center at Georgia State University
Mary Daniels
Executive Director, American College of Physicians Georgia Chapter
American College of Physicians
Jimmy Dills
Research Associate
Georgia Health Policy Center at Georgia State University
Sameera Fazili
Senior Visiting Adviser, Community and Economic Development
Federal Reserve Bank of Atlanta
Laurel Hart
Division Director, Housing Finance & Development
Georgia Department of Community Affairs
Harry Heiman
Director of Health Policy, Satcher Health Leadership Institute
Morehouse School of Medicine
Kathryn Lawler
Executive Director
Atlanta Regional Collaborative for Health Improvement (ARCHI)
Karen Leone de Nie
Assistant Vice President, Community and Economic Development
Federal Reserve Bank of Atlanta
Carol Lewis
President
Communities in Schools
Gary Nelson
President
Healthcare Georgia Foundation
Von Nguyen (Observer)
Acting Associate Director for Policy
Centers for Disease Control and Prevention
Jason O’Rouke
Senior Public Policy Director
Georgia Chamber of Commerce
Kathy Palumbo
Director of Programs
The Community Foundation
Michelle Rushing
Research Associate
Georgia Health Policy Center at Georgia State University
Meaghan Shannon-Vlkovic
Vice President and Market Leader, Southeast
Enterprise Community Partners
Bernita Smith
Director
Neighborhood Nexus/ARC
Courtney Smith
Vice President, Market Manager of Community Development Banking
PNC Bank
Shelley Spires
Chief Executive Officer
Albany Area Primary Health Care
Chris Thayer
Intern, Community and Economic Development
Federal Reserve Bank of Atlanta
Linda Wiant
Division Chief, Medical Assistance Plans
Georgia Department of Community Health